Airway Assessment
Imaging of the Airway Space with CBCT
Airway space assessment with a Large Field of View CBCT scanner will includes the following :
Nasal cavity
Nasopharynx
Oropharynx
Velopharynx
Hypopharynx
Below are some examples of anatomical airway concerns we routinely identify with iCAT 3-D imaging.
Nasal Airway:
- Nasal Valve Compromise (also referred to as nasal valve stenosis)
- Enlarged Turbinates (also referred to as turbinate hypertrophy)
- Concha Bullosa
- Suspected Deviated Septum (refer to ENT for diagnosis)
- Septal Bone Spur
- Enlarged Adenoids (often associated with mouth breathing)
- Enlarged Tonsils (often associated with mouth breathing)
- Chronic Sinusitis (often associated with mouth breathing)

1) Nasal Valve Compromise (or Stenosis): The arrows point to where the lateral walls of the nose are collapsed in and touching the cartilaginous septum of the anterior aspect of the nose. This narrowing of the nasal valve can increase resistance to nasal airflow.
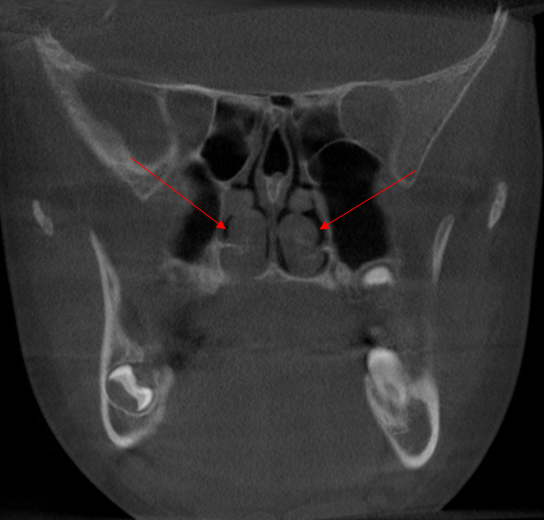
2) Enlarged Turbinates or Turbinate Hypertrophy: The arrows in the above image are pointing to the inferior turbinates near the back of the nasal airway. Enlarged turbinates can contribute to severe headaches and sleep disorder such as snoring and obstructive sleep apnea.

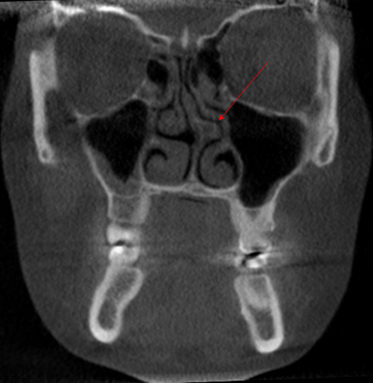
3) Conchae Bullosa: Concha Bullosa is also known as the middle turbinate. The arrows depict areas of the nasal cavity where the air pockets in the middle, turbinate.

4) Deviated Septum: We suspected this patient had a deviated septum so we referred to an ENT for diagnosis and treatment. Maxillary chronic sinusitis is also noted in this image.
5) Septal Bone Spur: A septal bone spur can cause significant airway obstruction and lead to turbulent nasal air flow and upper airway resistance. This patient was referred to an ENT for diagnosis and treatment.

8) Enlarged Adenoids:Mouth breathing can lead to the adenoids being hit with cold, dirty, and dry air. Enlarged adenoids are often a sign of mouth breathing and the adenoids often reduce in size with improving nasal breathing and/or improved tongue function (tongue resting at the roof of the mouth).

7) Enlarged Tonsils: In this axial view, it is apparent that the tonsils are encroaching on the narrow airway from both the right and left sides.

8) Chronic Sinusitis:The red arrow points to an area of chronic sinusitis. The yellow arrow points to a missing section of the maxillary sinus wall that was removed during a procedure called an antrostomy.
Pharyngeal Airway
With our 3-D software, we can create a volume rendering of the pharyngeal area and find the narrowest (most restricted) section of the airway which is called the ‘Minimum Cross-Sectional Area’ or MCA. We use this information to determine the risk of pharyngeal airway collapse during sleep. If a patient appears to be at an elevated risk of pharyngeal airway collapse during sleep and/or if a patient seems to have signs/symptoms related to airway obstruction, we will discuss a possible referral to medical colleagues for further evaluation. Please note that airway collapse is a multifactorial problem. There can be a patient with a small airway that does not collapse during sleep as well as patients with a large airway that does collapse during sleep. That is why we rely on our medical colleagues and sleep tests for proper diagnosis.
Figure 1: This is an axial view of an extremely narrow pharyngeal airway with an MCA of 10 mm2. Due to the severely narrow airway and a medical history that included chronic orofacial pain, this patient was referred for a sleep study and diagnosed by a sleep physician with severe sleep apnea.

Figure 2: This is a sagittal view of a large pharyngeal airway with an MCA of roughly 400 mm2. This patient would be considered at low risk of an SBRD related to airway collapse. However, a complete screening includes checking for other signs and symptoms of airway obstruction.
